Shoulder Labrum tears can be a scary and tricky injury to deal with. In this discussion we will cover the anatomy of the shoulder joint, the types of shoulder labrum tears, the causes of tearing, how to diagnose a labral tear, treatment options available, and rehab protocols for a tear of the shoulder labrum.
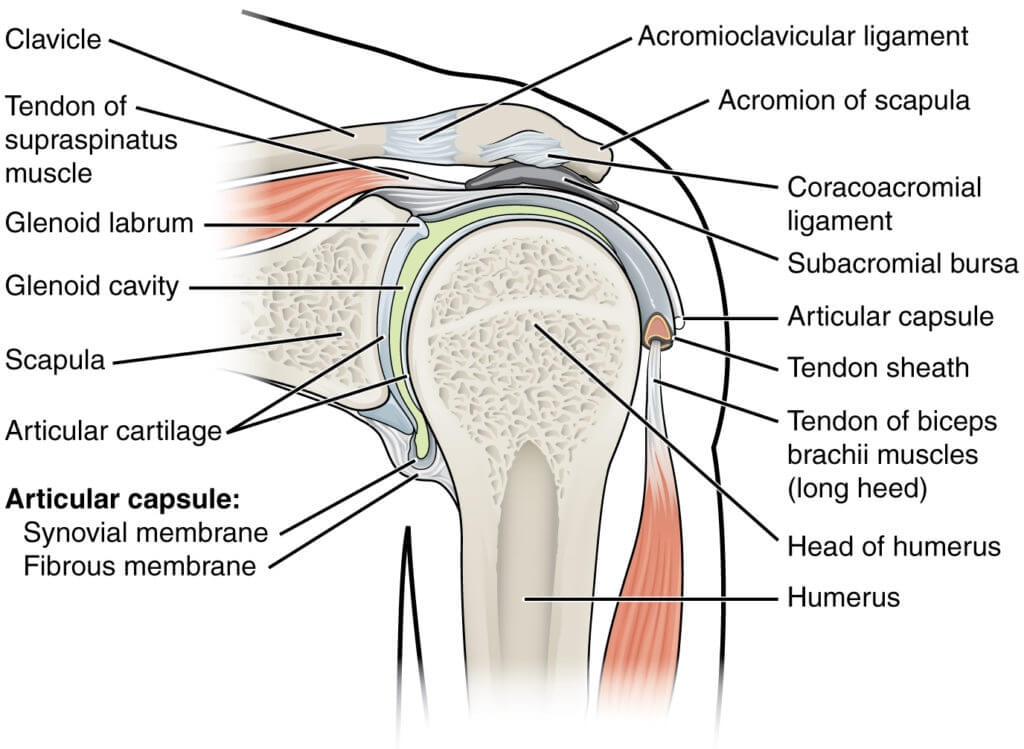
Table of Contents
Shoulder Joint Anatomy
The shoulder joint is located where the Humerus, Scapula, and Clavicle meet. The shoulder joint is considered a ball and socket joint. The glenoid fossa of the scapula is the socket of the joint and the head of the humerus is the ball of the joint. The glenoid fossa (socket) is shallow when compared to the acetabulum (socket) of the hip. This shallowness provides the large range of motion that we have within the shoulder joint. However, with this range of motion, comes a sacrifice to stability within the joint. This is where the labrum comes into play.
The glenoid labrum of the shoulder joint is a cup-shaped rim of cartilage that lines and reinforces the glenoid labrum and provides stability to the shoulder. The labrum also acts as an attachment site for many of the shoulder ligaments, muscles, and tendons. Unfortunately, because of the labrums role in providing stability and attachment for these structures, injury to the labrum can cause instability, pain, popping, clicking, catching, and/or the feeling of possible dislocation within the shoulder.
Types of Labral Tears
The two most common types of labral tears that we see are SLAP (superior labrum from anterior to posterior) tears and Bankart tears. However, anterior and posterior tears are possible as well. These tears are usually accompanied by aching pain and difficulty performing normal shoulder movements.
SLAP Tear
SLAP tears occur at the area of the labrum where the bicep tendon attaches. These tears are common in baseball pitchers and volleyball server/spikers because of their dynamic, high-energy and whip-like overheard movement pattern. These injuries are typically accompanied by pain at the location of the bicep tendon insertion at the labrum and a feeling of instability.
Bankart Tear
Bankart tears typically occur in younger athletes who have dislocated their shoulder. When the shoulder dislocates, it sometimes pulls the lower portion of the labrum with such a force that it causes tearing. These types of tears can commonly lead to multiple dislocations if not treated or rehabbed correctly.
Causes of Labral Tears
Labral tears are caused by Acute injuries (trauma/blunt force) or Chronic injuries (repetitive/Overuse/Misuse). Acute injuries are often seen in the form of a fall on an outstretched arm, a motor vehicle accident with hands on the wheel, heavy lifting or blows to the shoulder. Chronic injuries can occur from repetitive motion patterns such as baseball pitching or volleyball serving and spiking.
Diagnosing Labral Tears
The best way to diagnose a labral tear is to seek medical evaluation by an orthopedic, chiropractic or physical therapist physician that is well versed in sports injury and athletic mechanics. These practitioners will most commonly perform a series of orthopedic examinations to diagnose the problem. The most common tests that you will find are the O’Briens, Jerk, and Jobes test. If the physician determines that there may be a labral tear, further imaging is usually recommended to confirm the diagnosis. Typically an MR Arthrogram or an MRI is in order at this time.
O’Brien’s Test


A positive O’Briens Test is indicative of a potential SLAP Tear.
- With the patient positioned in a sitting or standing position, the upper extremity to be tested is placed in 90° of shoulder flexion and 10-15° of horizontal adduction
- The patient then fully internally rotates the shoulder and pronates the elbow
- The examiner provides a distal stabilizing force as the patient is instructed to apply an upward force
- The procedure is then repeated in a neutral shoulder and forearm position
- A positive test occurs with pain reproduction or clicking in the shoulder with the first position and reduced/absent with the second position
- Depth of symptoms must also be assessed as superficial pain can indicate acromioclavicular joint symptoms and deep pain is more often a sign of a labral lesion
Jerk Test


A positive Jerk Test is indicative of a potential posterior-inferior labral tear or lesion or posterior-inferior instability of the shoulder complex.
- Stabilize the patient’s scapula with one hand and hold the affected arm at 90° abduction and internal rotation
- The examiner grasps the elbow and axially loads the humerus in a proximal direction
- The arm is moved horizontally across the body.
- A positive result is indicated by a sudden clunk as the humeral head slides off the back of the glenoid
- When the arm is returned to the original position, a second jerk may be observed, that of the humeral head returning to the glenoid
Jobe’s Apprehension-Relocation Test


A positive Jobe’s Test is indicative of potential anterior instability of the shoulder joint complex.
- With the patient positioned supine, with the elbow flexed to 90 degrees and abducted to 90 degrees
- The therapist then applies an external rotation force to the shoulder, if the patient reports apprehension in any way, the Apprehension Test is considered to be positive.
- At this point, the therapist may apply a posteriorly directed force to the shoulder – if the patient’s apprehension or pain is reduced in this position, the Jobe Relocation Test is considered to be positive
- It is important to note that the therapist should always bring the arm back into a neutral position before releasing the relocation force (posterior glide of the head of the humerus) for risk of shoulder dislocation.
Treatment of Labral Tears
Labral tears are treatable both conservatively or surgically. Our recommendation is to alway treat conservatively prior to surgically, however it is always your decision. Conservative treatment typically comes in the form of anti-inflammatory medications, steroid injections, exercise rehabilitation methods, and soft tissue therapies such as massage, instrument assisted soft tissue mobilization, myofascial release technique, and cupping. In a case where conservative treatment methods do not provide a solution or come to a halt, surgical intervention may be necessary.
Surgical intervention typically involves arthroscopic surgery to repair and re-attach the torn aspects of the labrum with anchors and sutures.
Rehab Protocol for Labral Tear – Conservative
Rest
A period of rest is necessary for properly healing and rehabbing most types of injuries. In this case rest does not mean halting motion of the joint all together, but instead, it means an avoidance of exercises and motions that aggravate the joint and/or cause pain.
Phase I: Rehab Weeks 1 – 4
In the first weeks of rehab it is a good idea to incorporate rest and avoidance of pain and aggravation within the shoulder joint as well as proper stretching. The idea is to stretch and mobilize the joint to restore full range of motion in all directions being sure to always stop just prior to pain. During this phase we also need to avoid loading of the bicep tendon which attaches directly to the labrum so that further damage does not occur.


During this phase we also want to activate and strengthen the stabilizer muscles of the shoulder joint proper and the scapula. These muscles include the trapezius, serratus anterior and the muscles of the rotator cuff (supraspinatus, teres minor, infraspinatus, subscapularis). During this phase, focus on subtle loading with moderate to high repetitions as well as controlled movement.
- Forward flexion in a side lying position
- Prone extension
- Horizontal row
- Serratus press
- Modified push-up with a plus
- Internal rotation in 20 and 90 degrees of abduction
- External rotation in 20 and 90 degrees of abduction







Phase II: Rehab Weeks 5 – 12
- Short lever forward flexion in external rotation with forearm supination
- Long lever forward flexion in external rotation with forearm supination
- Full can
- Elbow flexion with forearm supination
- Uppercut
In this phase we will start subtle loading of the biceps. Progressing load gradually throughout the weeks of phase II. At this point we can begin progressing into further motion of the phase I stretches.
Phase III: Rehab Weeks 13 – 16
Phase III consists of sport specific exercise and movements. This phase varies depending on your sport, activities, and/or goals. During this phase it is a good idea to warm-up the shoulder using phase II protocol prior to starting your sport specific exercise.
Thoracic and Cervical Mobility and Stability
The movement patterns of the shoulder are directly related to mobility and stability of the thoracic and cervical spine. Therefore, the thoracic and cervical spine should not be ignored when rehabbing shoulder injuries. For more info on thoracic mobility with a foam roller, visit this post! Thoracic Mobility With A Foam Roller


